
Double checking of medication is normal practice for many medicines in the UK, particularly controlled drugs which is a mandatory process. However, there is no legal requirement for this to happen with non-controlled drugs, although many trusts require certain drugs to be double checked as part of their medicines policy.
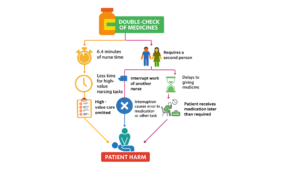
Around 130,000 medication mistakes happen every day in NHS hospitals. Most of these mistakes happen when medicines are being given to patients (e.g. wrong medicine, wrong dose, wrong patient). These errors are common and can harm patients and in rare cases, can lead to serious injury or death. ‘Double checking’ a medicine before giving it to the patient is often used to reduce medication errors. However, there is no convincing evidence that it works. Research on paediatric wards in Australia (Westbrook, 2021) showed nurses spent a lot of time double checking (6.4 minutes per check) which could actually cause harm to patients by causing delays to them getting critical medicines. Across the NHS, based on these findings, there could be an estimated to cost between £412 million and £1.28 billion each year.
If double-checking clearly improved patient safety, this time and cost might be worthwhile. But evidence suggests that double-checking is often not carried out properly, may not work as intended, and can sometimes even contribute to harm. Because of this, nurses’ time might be better used on other safety activities that more effectively improve patient care.
In 2022, NHS England identified the question “Does double-checking medicines reduce errors?” as a national research priority. Our study aims to answer this question.
The NIHR Yorkshire and Humber Patient Safety Research Collaboration, were awarded funding to research this question. We have worked with patients and healthcare staff to better understand the issue and how often double-checking is used. We found that double-checking medicines is common in hospitals across England, although only a few hospitals have tried to reduce or stop the practice. Both staff and patients agreed that reducing low-value care is important for improving modern healthcare.
This work is split into 5 smaller projects detailed below.










